In the vast majority of cases floaters are harmless and represent the normal, natural (although occasionally annoying) ageing change of the eye. They usually become much less obvious with time as the brain adjusts to the change and eventually filters them out.
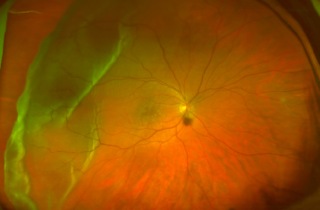
Very rarely during the development of a posterior vitreous detachment, the vitreous gel can be stuck to a patch of retina and cause a retinal tear. A retina tear can occur in up to 10% of PVD patients. If the seal of the retina against the back of the eye is broken, fluid can start to track in behind the retina causing it to detach from the back of the eye a little like wallpaper peeling of a wall. A retinal detachment is an uncommon event that occurs in approximately 1 in 10,000 of the population in general. Usually, if a tear develops in the retina people experience a very marked shower of floaters associated with flashes of light in their peripheral vision. The light is usually persistent and occurs in daylight. Some people notice a curtain effect coming in from their peripheral visual field. This requires urgent attention by an eye doctor.
In a different situation, the vitreous detachment can pull on a retinal blood vessel, and if the blood vessel is broken then the vitreous jelly fills with blood, and this is called a vitreous haemorrhage. A small shower of spots in your vision suggests a mild amount of blood in the vitreous. If you see large dark blobs in your vision or if your vision is generally very hazy or blurred, then this suggests a much larger haemorrhage in the vitreous jelly.