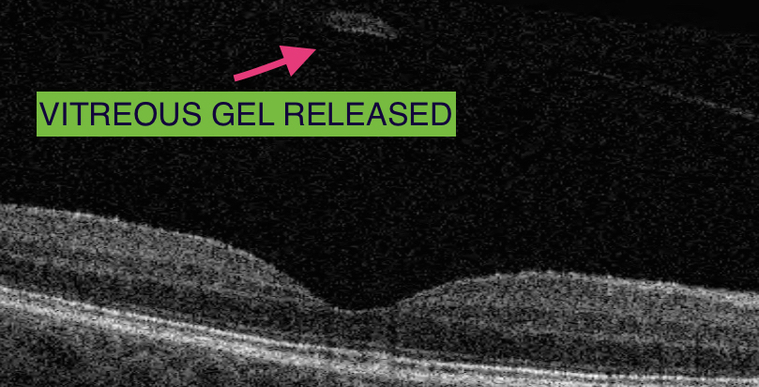
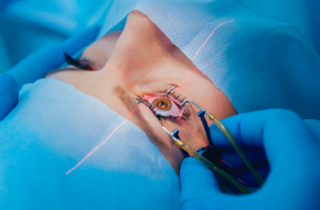
Vitrectomy surgery can be performed under local anaesthetic or general anaesthetic, and does not usually take longer than an hour. It can be performed using a local anaesthetic injection with the patient remaining comfortable and awake during the procedure. It is very important for the patient to stay still, especially during the very delicate manoeuvres when the vitreomacular traction is removed from the centre of the macula. The vitreous is replaced by natural aqueous fluid produced inside the eye. In some cases, the surgeon has to leave a special gas bubble inside the eye which disappears on its own after a few weeks.
Following treatment of vitreomacular traction, the vision is typically more blurred and it can take months for it to improve. The Surgery is usually successful in reducing the distortion in vision due to the vitreomacular traction. If the vision had not been distorted prior to vitreomacular traction release, improvement in the sharpness of vision and reading is less predictable.