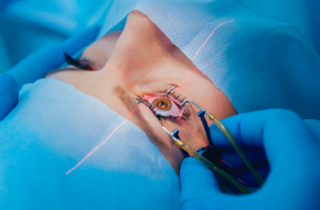
A macular hole can often be repaired by an operation called a Vitrectomy, peel and gas. As cataract is inevitable, you may be offered combined vitrectomy surgery with cataract extraction and lens implantation (‘phacoemulsification”) at the same time as the macular hole repair.
If the hole has been present for less than a year, the surgery will be successful in closing the hole in about 90% of cases. Of these, more than 70% will be able to see two or three lines more down a standard vision chart, compared to before the surgery. Even if this degree of improvement does not occur, the vision is at least stabilised and many patients find that they have less distortion.
In a minority of patients the hole does not close despite surgery and the central vision can continue to deteriorate; however, a second operation can still be successful in closing the hole. It is important to understand that return to completely normal vision is not possible.
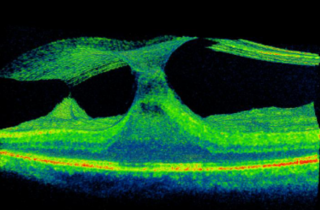
For patients with small macular holes with “vitreomacular traction“, an injection of a therapeutic drug called Ocriplasmin may be successful in closing the macular hole without the patient requiring a surgical operation. The drug loosens the “jelly” within the eye known as the vitreous. The jelly then softens and peels away from the surface of the macula, and in the process, the macular hole can close. Vitrectomy surgery is far superior to this drug, but some patients with small macular holes may wish to avoid an eye operation so “intravitreal ocriplasmin” may be their choice of treatment. Please discuss this with your surgeon Mr Muqit, and he will discuss the natural history of small macular holes with you, together with both conservative and treatment options.